
80 yr old male presents to HUM with shortness of breath and this EKG. What’s going on, and what must you do IMMEDIATELY to treat him appropriately?

Peaked T-waves in Hyperkalemia From: Lifeinthefastlane.com
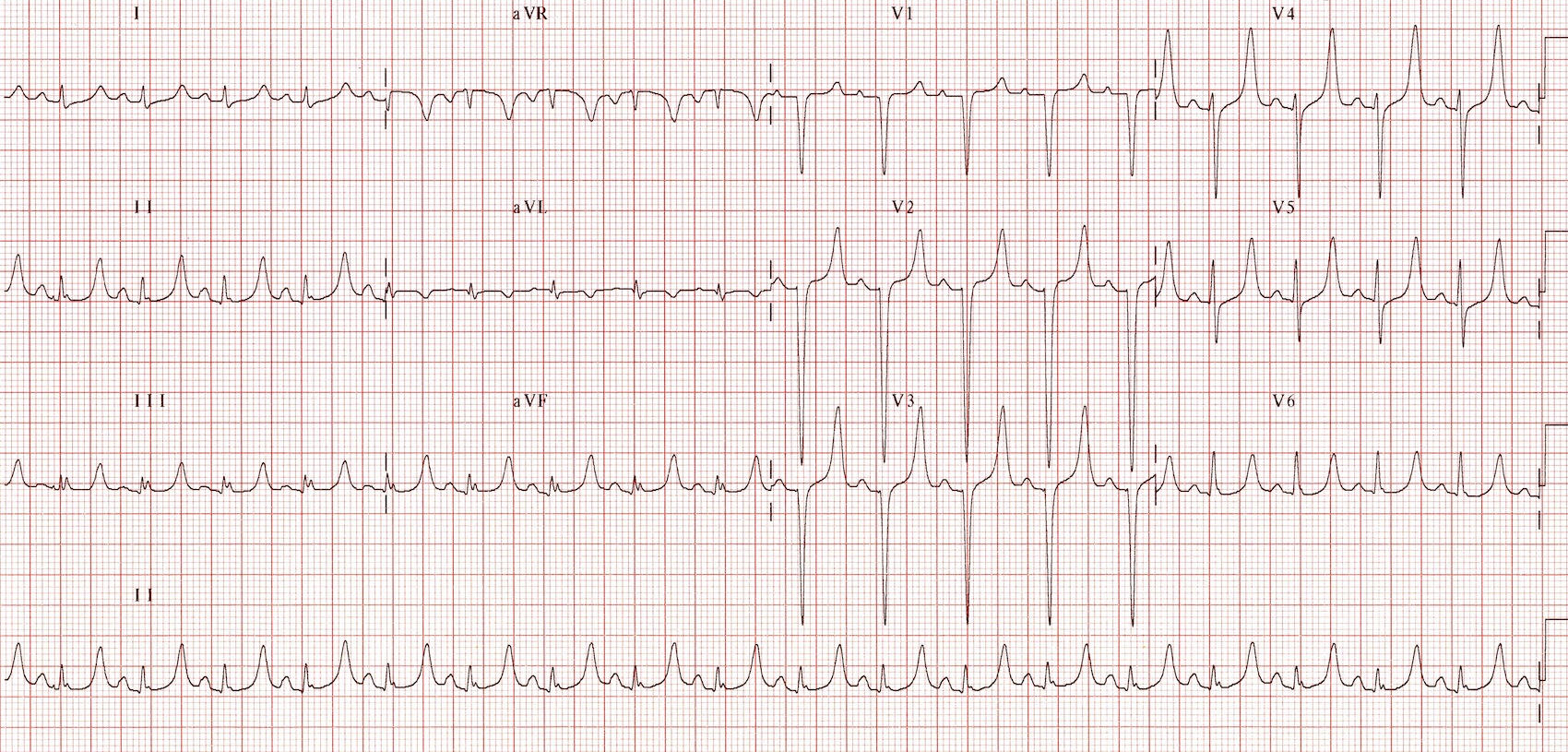
This EKG is highly specific if not almost certainly abnormal due to HYPERKALEMIA. While peaked T-waves (remember that they should be evident in almost ALL leads!) are the earliest sign of hyperkalemia and can occur with potassium levels as low as 5.5 mEq/L, this patient’s EKG suggests a far higher level of serum potassium.
With rising potassium levels, EKG changes generally occur in the following order:
- –Peaked T waves
- –Prolonged PR
- –Prolonged QRS
- –Loss of p wave
- –Sine wave pattern
- –Sinus Arrest
What is remarkable about this EKG is that in the short time that it was performed, we were able to witness the rapid progression of these signs:
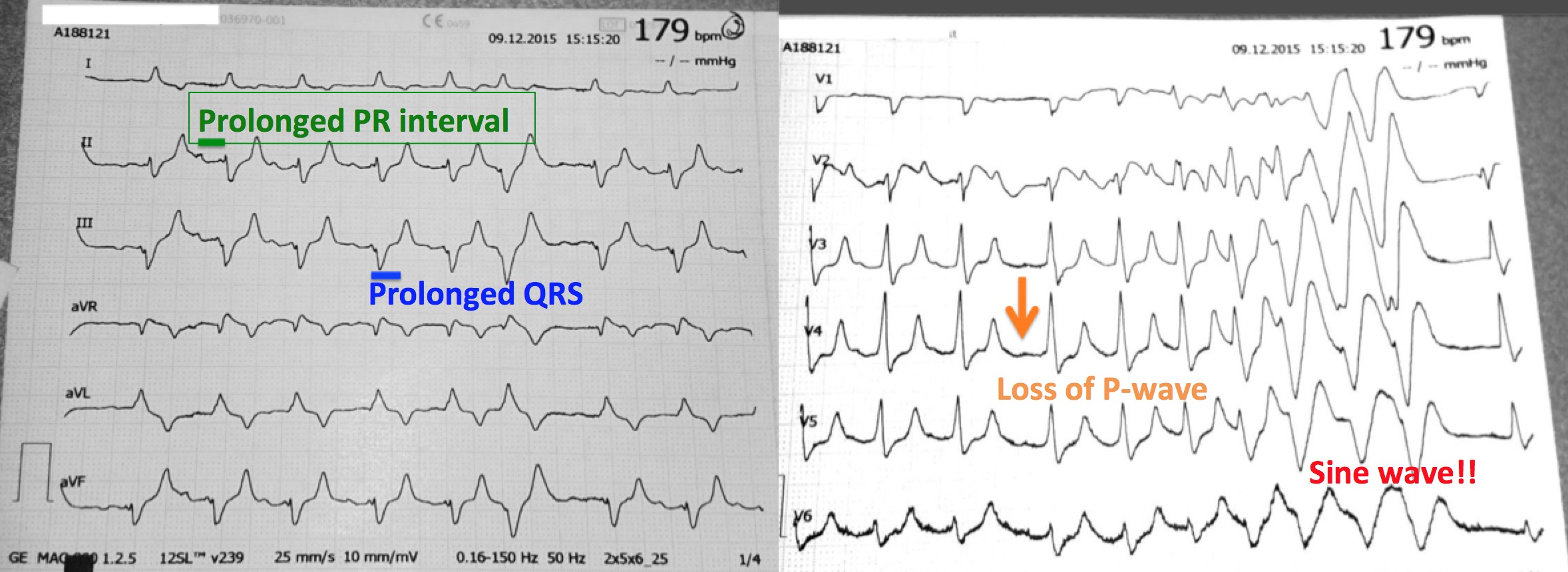
This patient is heading toward cardiac arrest and must be treated IMMEDIATELY!
So how do we treat:
Stabilize the myocardium:
- Calcium – (Calcium gluconate 1 – 2mg over 2 – 3 minutes) Stabilizes the myocardium and should be the first thing administered.
Lower the serum potassium by pushing K into cells:
- Insulin and Dextrose (to prevent hypoglycemia) – can give 5 – 10 units of insulin and 1 amp of D50.
- Bicarbonate – 50 – 200mmol of 8.4% sodium bicarb (amp are typically 1mmol/ml and come in 50 – 100ml vials, if severe like this patient put 1 – 2 amps in 500cc – 1000cc of NaCl and start infusing)
- Salbutomol – just start nebulizing
Lower total body potassium!!:
While we have lowered the serum potassium, we have not yet done anything to ensure that the patient’s total body potassium will decrease. We have only temporarily hidden the potassium inside cells. In these cases, it is essential that the patient is making urine. IF THE PATIENT IS NOT MAKING URINE, THEN HE OR SHE WILL NEED DIALYSIS!! Make sure the patient is on a monitor, has 2 good IVs and has a FOLEY to monitor output, consider furosemide to increase output, and kayexalate to absorb potassium through the GI tract.
Once you have done that…you can start thinking again about your other patients because with his nurse closely monitoring and with the salbutomal still smoking away, you know, whatever happens, that at least you’ve done the best you could.
Links:
Life in the Fast lane – ECG changes Hyperkalemia
Emcrit podcast on treatment of severe hyperkalemia
Weisberg LS. Management of severe hyperkalemia. Crit Care Med. 2008 Dec;36(12):3246-51.
